The Kidneys: Structure, Function, and Health
Introduction
 Behind the spine, in retroperitoneal darkness, rest two bean-shaped organs each containing one million irreplaceable nephrons—filtering the entire blood volume forty times daily, transforming 180 liters of plasma into exquisitely calibrated urine while maintaining pH at 7.40, sodium at 140 mEq/L, potassium at 4.0 mEq/L with molecular precision separating consciousness from coma. These 150-gram structures receive 1,200 milliliters of blood per minute—one-quarter of cardiac output—executing filtration, reabsorption, secretion, and endocrine synthesis that defends the infinitesimally narrow chemical composition permitting cellular metabolism. In the seconds required to read this sentence, they have already saved life three times over.
Behind the spine, in retroperitoneal darkness, rest two bean-shaped organs each containing one million irreplaceable nephrons—filtering the entire blood volume forty times daily, transforming 180 liters of plasma into exquisitely calibrated urine while maintaining pH at 7.40, sodium at 140 mEq/L, potassium at 4.0 mEq/L with molecular precision separating consciousness from coma. These 150-gram structures receive 1,200 milliliters of blood per minute—one-quarter of cardiac output—executing filtration, reabsorption, secretion, and endocrine synthesis that defends the infinitesimally narrow chemical composition permitting cellular metabolism. In the seconds required to read this sentence, they have already saved life three times over.
Main Article
The kidneys constitute biological masterworks where physics, chemistry, and cellular intelligence converge to defend life's narrow chemical boundaries against entropic dissolution. Each kidney houses approximately one million nephrons—irreplaceable functional units incapable of regeneration after birth, rendering every one precious beyond calculation. These microscopic structures generate a glomerular filtration rate averaging 125 milliliters per minute in healthy adults, producing 180 liters of ultrafiltrate daily from which 99% undergoes meticulous reabsorption, yielding 1-2 liters of final urine whose composition varies continuously based on hydration status, dietary intake, metabolic activity, and endocrine signaling. This extraordinary processing volume—180 liters filtered, 178 liters recovered—reveals the kidneys' defining paradox: creating massive filtrate to achieve exacting control, filtering everything to selectively salvage what sustains while eliminating what threatens.
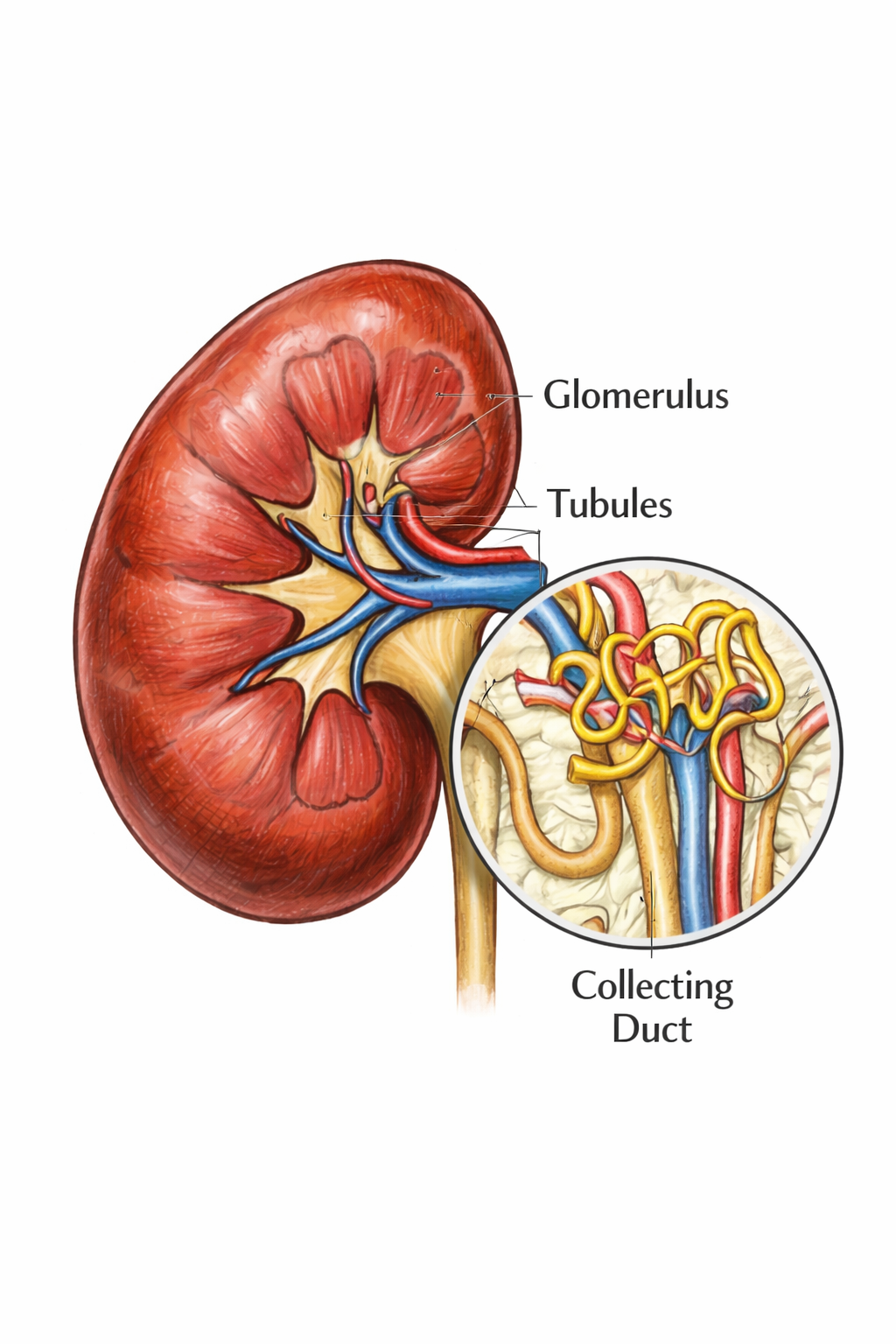
The nephron's architecture demonstrates evolutionary perfection refined across 500 million years of vertebrate history. Blood enters through the afferent arteriole into the glomerulus—a spherical capillary network featuring fenestrated endothelium, negatively-charged basement membrane, and podocyte filtration slits creating a molecular sieve permitting water, electrolytes, glucose, amino acids, and molecules below 7 kilodaltons while retaining albumin and larger proteins based on molecular size and electrical charge. Starling forces govern this ultrafiltration with mathematical elegance: glomerular capillary hydrostatic pressure (60 mmHg) drives fluid outward against Bowman's capsule hydrostatic pressure (15 mmHg) and plasma oncotic pressure (29 mmHg), yielding net filtration pressure approximating 16 mmHg. This pressure-driven mechanism requires no cellular energy expenditure yet achieves exquisite molecular selectivity through size exclusion and charge repulsion—passive physics accomplishing what active processes cannot replicate, operating continuously in structures invisible to unaided vision.
Filtrate enters the proximal convoluted tubule where epithelial cells bristling with millions of apical microvilli forming extensive brush borders reabsorb 65% of filtered sodium and water through basolateral Na⁺/K⁺-ATPase pumps establishing electrochemical gradients driving secondary active transport of countless solutes simultaneously. Sodium-glucose cotransporters—SGLT2 dominating early proximal segments, SGLT1 operating in late segments—reclaim approximately 180 grams of glucose daily with efficiency so absolute that zero grams appear in normal urine until plasma glucose exceeds the tubular transport maximum near 180 milligrams per deciliter, whereupon glycosuria ensues. Sodium-dependent amino acid transporters recover filtered proteins completely, preventing any loss. Bicarbonate reabsorption reclaims 4,500 milliequivalents daily through carbonic anhydrase converting filtered bicarbonate and secreted hydrogen ions into carbon dioxide and water, which diffuse into cells, regenerate bicarbonate for basolateral transport into blood, and maintain systemic pH homeostasis within the narrow 7.35-7.45 range where deviation by 0.4 units in either direction proves incompatible with consciousness. This proximal recovery operates continuously, automatically, flawlessly—preventing catastrophic nutrient losses that would otherwise prove fatal within days of complete kidney failure.
The loop of Henle descends deep into the renal medulla executing countercurrent multiplication—an engineering achievement creating the osmotic gradient enabling urine concentration reaching 1,200 milliosmoles per kilogram, quadruple plasma osmolality, conserving water during states of dehydration. The thin descending limb exhibits high water permeability via aquaporin-1 channels but negligible solute permeability, releasing water into the hypertonic medullary interstitium and progressively concentrating tubular fluid as it descends. The thick ascending limb reverses this arrangement completely: the Na⁺-K⁺-2Cl⁻ cotransporter actively extracts ions without accompanying water while remaining absolutely water-impermeable, diluting tubular fluid while simultaneously increasing interstitial osmolality progressively. This countercurrent architecture—parallel tubular segments with opposite permeability characteristics flowing in opposite directions—generates and maintains the medullary gradient permitting facultative water conservation during dehydration or rapid water excretion during overhydration, responding within hours to changing physiological demands through mechanisms refined across evolutionary time.

The distal convoluted tubule performs hormone-regulated electrolyte fine-tuning under precise aldosterone influence and parathyroid hormone control. The thiazide-sensitive Na⁺-Cl⁻ cotransporter reabsorbs sodium chloride under hormonal regulation. Parathyroid hormone stimulates TRPV5 calcium channels increasing calcium reabsorption when serum calcium falls below physiological ranges. Magnesium transport occurs through claudin-16 paracellular pathways and TRPM6 apical channels responding to magnesium status. This segment translates circulating endocrine signals into precise tubular transport adjustments matching systemic metabolic requirements moment-to-moment, executing the body's chemical commands with molecular fidelity.
The collecting duct determines final urine composition through two specialized cell types executing opposite functions with flawless coordination. Principal cells express epithelial sodium channels (ENaC) reabsorbing sodium under aldosterone control while simultaneously secreting potassium through ROMK channels, and contain aquaporin-2 water channels inserted into apical membranes when vasopressin binds V2 receptors, activating protein kinase A signaling pathways enabling water reabsorption that concentrates urine during dehydration or water restriction. Type A intercalated cells secrete hydrogen ions via vacuolar H⁺-ATPase pumps, acidifying urine to pH 4.5 and generating new bicarbonate replacing that consumed buffering metabolic acids from protein catabolism. Type B intercalated cells secrete bicarbonate through pendrin chloride-bicarbonate exchangers, alkalinizing urine when systemic alkalosis requires correction. This dual-cell system provides bidirectional acid-base regulation impossible with uniform cellular architecture, enabling dynamic pH control across physiological and pathological states.
Beyond filtration and reabsorption, kidneys actively secrete substances from peritubular capillary blood into tubular fluid for definitive elimination. Organic anion transporters (OAT1, OAT3) and organic cation transporters (OCT2) in proximal tubules secrete drugs, toxins, and metabolites achieving clearances exceeding glomerular filtration rate—definitive proof of active secretion powerfully supplementing passive filtration. Potassium secretion in collecting ducts adjusts dynamically to dietary intake: high potassium consumption triggers aldosterone secretion increasing ENaC-mediated sodium reabsorption, hyperpolarizing principal cells, opening ROMK potassium channels, and enhancing secretion within hours of ingestion, preventing the potentially fatal hyperkalemia that would otherwise ensue. Hydrogen ion secretion throughout all nephron segments enables net acid excretion of 50-100 milliequivalents daily, precisely matching metabolic acid production from dietary protein catabolism with atomic precision.
The kidneys function as sophisticated endocrine organs producing hormones affecting distant tissues fundamentally throughout the organism. Erythropoietin synthesis by peritubular interstitial fibroblasts responds to tissue hypoxia detected through oxygen-sensitive prolyl hydroxylase enzyme systems: adequate oxygen permits hydroxylation of hypoxia-inducible factor-alpha, targeting it for proteasomal degradation and preventing transcription; hypoxia inhibits hydroxylation, stabilizing HIF-alpha, which translocates to nuclei transactivating erythropoietin genes, increasing plasma concentrations within hours and stimulating bone marrow red blood cell production within days, correcting anemia and restoring tissue oxygen delivery. Renin secretion from juxtaglomerular cells initiates the renin-angiotensin-aldosterone cascade controlling blood pressure and sodium balance systemically: renin enzymatically cleaves hepatic angiotensinogen forming angiotensin I, converted by pulmonary endothelial angiotensin-converting enzyme to angiotensin II—the body's single most potent vasoconstrictor—which elevates blood pressure through systemic arterial constriction, stimulates adrenal cortex aldosterone secretion increasing distal nephron sodium reabsorption, raises circulating blood volume, and enhances sympathetic nervous activity. The enzyme 1-alpha-hydroxylase in proximal tubule mitochondria converts hepatic 25-hydroxyvitamin D3 to 1,25-dihydroxyvitamin D3 (calcitriol), stimulated by parathyroid hormone and hypophosphatemia, enabling intestinal calcium absorption essential for skeletal mineralization, neuromuscular transmission, cardiac contractility, and immune system competence—demonstrating profound renal endocrine control over mineral metabolism, erythropoiesis, and cardiovascular regulation extending far beyond simple waste filtration and elimination.
Function
Kidney function integrates four fundamental processes—glomerular filtration, tubular reabsorption, tubular secretion, and endocrine synthesis—into unified homeostatic regulation defending extracellular fluid composition against the constant assault of metabolism, ingestion, and cellular death. These processes operate simultaneously with molecular precision unmatched by any human-engineered technology.
Filtration initiates as hydrostatic pressure drives plasma through the glomerular filtration barrier comprising three distinct layers: fenestrated endothelium with 70-90 nanometer pores allowing plasma passage, basement membrane containing negatively-charged glycoproteins restricting anionic proteins, and podocyte foot processes forming 25-60 nanometer filtration slits bridged by nephrin-based diaphragms. This trilaminar architecture creates size-selective and charge-selective ultrafiltration permitting molecules below 7 kilodaltons while restricting albumin and larger proteins effectively. Autoregulation maintains stable glomerular filtration rate across mean arterial pressures ranging 80-180 mmHg through two mechanisms: myogenic responses where afferent arterioles contract when stretched by increased intraluminal pressure, and tubuloglomerular feedback where macula densa cells sense elevated distal tubule sodium chloride delivery, releasing adenosine and ATP that constrict afferent arterioles preventing excessive filtration and nutrient loss.
Reabsorption recovers filtered substances through transcellular pathways—crossing apical membranes into cells then basolateral membranes into blood via specific transporters—and paracellular pathways passing between cells through claudin-based tight junction pores driven by electrochemical gradients. Active transport mechanisms driven by primary Na⁺/K⁺-ATPase pumps and secondary cotransporters or exchangers recover sodium, glucose, amino acids, bicarbonate, phosphate, and other essential solutes with near-perfect efficiency.
Secretion actively transports substances from peritubular capillary blood into tubular lumen through organic anion transporters, organic cation transporters, potassium channels, and hydrogen ion pumps, enabling clearance of drugs, environmental toxins, excess potassium, and metabolic acids beyond what filtration alone achieves. Endocrine functions include erythropoietin synthesis stimulating bone marrow red blood cell production preventing anemia, renin secretion initiating systemic blood pressure regulation through angiotensin-aldosterone pathways, and calcitriol production enabling intestinal calcium absorption necessary for skeletal health. These integrated processes execute continuous adjustments maintaining volume, osmolality, pH, and electrolyte concentrations within narrow physiological ranges absolutely essential for enzymatic activity, membrane potentials, and cellular viability.
Structural Organization
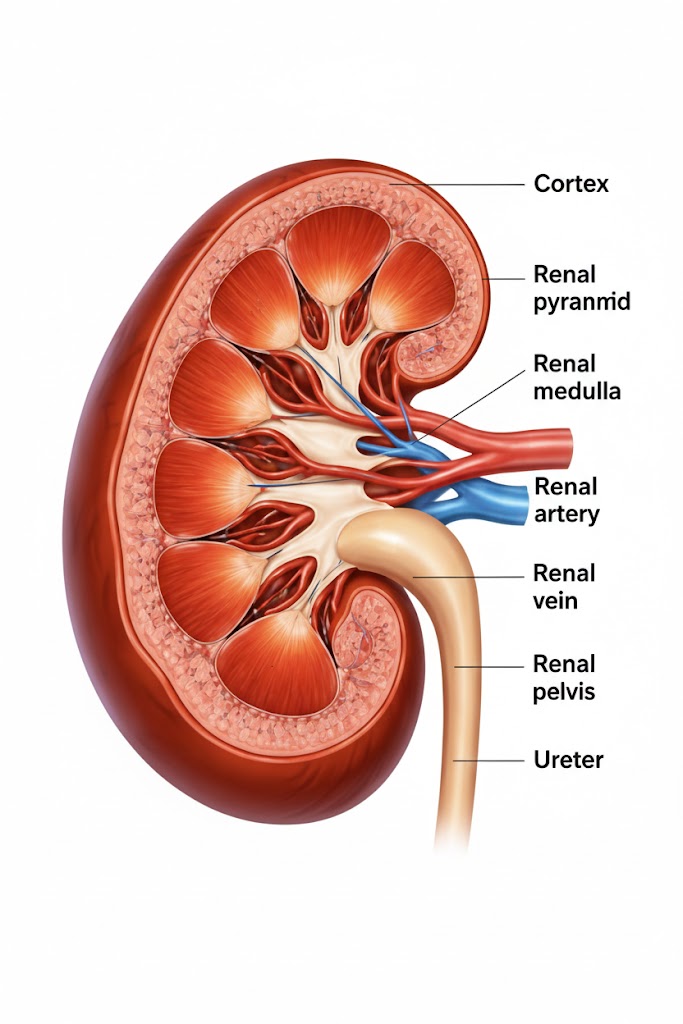
The kidney's gross anatomy divides into distinct cortex and medulla regions surrounded externally by tough fibrous capsule providing structural integrity. The cortex—appearing reddish-brown and granular containing all glomeruli, proximal convoluted tubules, distal convoluted tubules, and cortical collecting ducts arranged densely—receives approximately 90% of renal blood flow supporting intensive filtration and reabsorption processes. The medulla consists of 8-12 cone-shaped renal pyramids with broad bases facing cortex and pointed apices called papillae projecting into minor calyces where urine drainage begins. Pyramids contain precisely parallel arrays of loops of Henle and medullary collecting ducts creating the essential architectural substrate for countercurrent multiplication mechanisms generating medullary hypertonicity enabling urinary concentration.
The nephron—representing the kidney's irreplaceable functional unit—comprises two major components: the renal corpuscle where blood filtration occurs and the renal tubule where filtrate modification happens. The corpuscle contains the glomerulus, a specialized capillary network formed by afferent arteriole division into 4-8 capillary loops that reunite forming the efferent arteriole, surrounded by Bowman's capsule collecting filtered fluid. The tubule extends through sequential segments: proximal convoluted tubule performing bulk reabsorption through cells bearing extensive apical microvilli maximizing surface area; descending thin limb highly permeable to water via aquaporins; ascending thick limb water-impermeable while actively transporting sodium, potassium, and chloride generating dilute urine and concentrated medullary interstitium; distal convoluted tubule performing hormone-regulated fine-tuning of electrolyte composition; and collecting duct making final adjustments under vasopressin and aldosterone control determining whether final urine becomes dilute or concentrated.
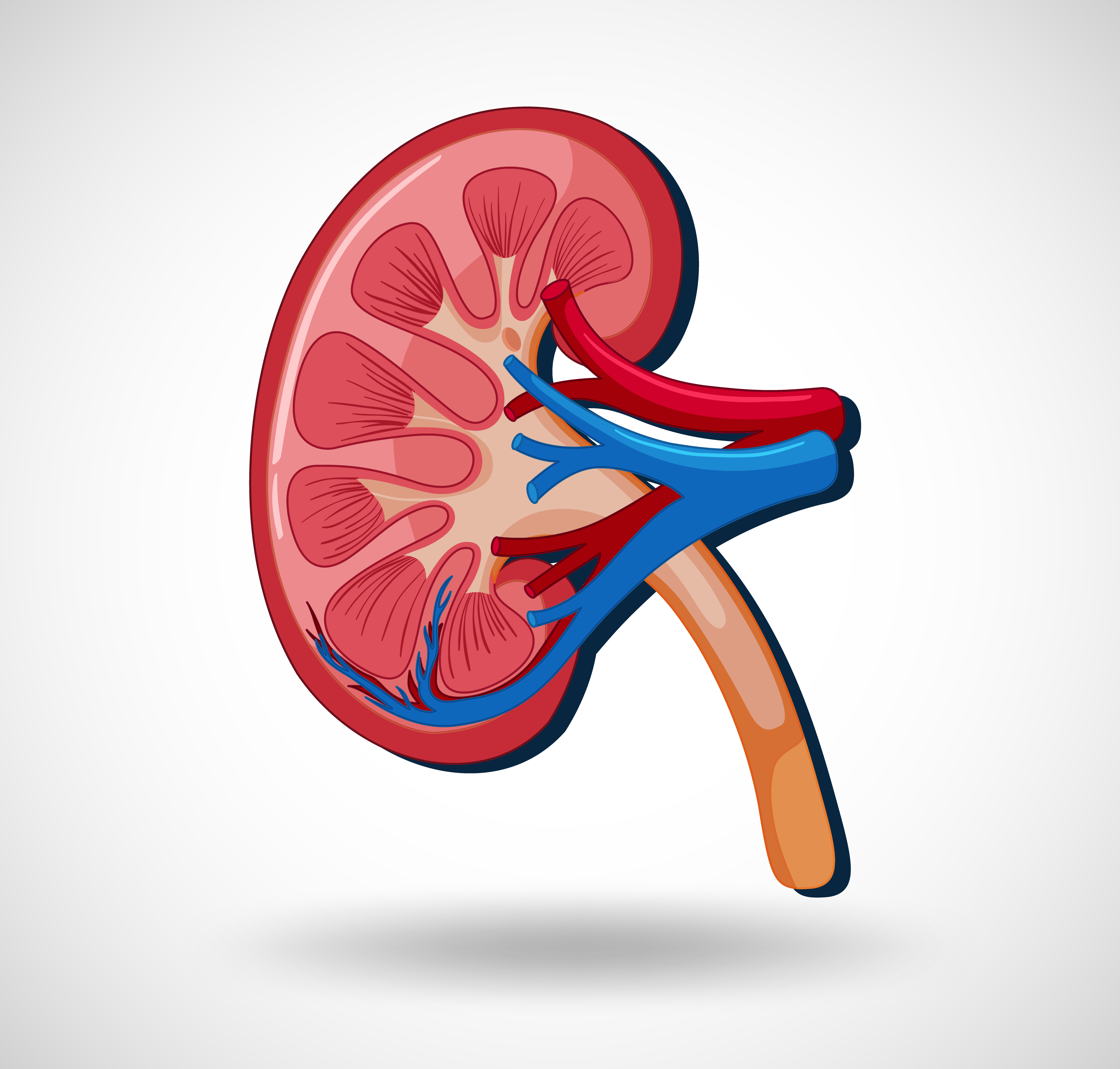
 Renal blood supply follows stereotyped hierarchical branching: renal artery dividing into segmental arteries, interlobar arteries ascending between pyramids toward cortex, arcuate arteries arching along the corticomedullary junction, interlobular arteries radiating perpendicular into cortex, afferent arterioles supplying individual glomeruli for filtration, efferent arterioles forming peritubular capillaries surrounding cortical tubules or vasa recta paralleling medullary loops enabling reabsorption. This unique dual capillary arrangement—high-pressure glomerular filtration followed by low-pressure peritubular reabsorption—enables maximally efficient blood processing unmatched by single-capillary systems, refined across evolutionary time.
Renal blood supply follows stereotyped hierarchical branching: renal artery dividing into segmental arteries, interlobar arteries ascending between pyramids toward cortex, arcuate arteries arching along the corticomedullary junction, interlobular arteries radiating perpendicular into cortex, afferent arterioles supplying individual glomeruli for filtration, efferent arterioles forming peritubular capillaries surrounding cortical tubules or vasa recta paralleling medullary loops enabling reabsorption. This unique dual capillary arrangement—high-pressure glomerular filtration followed by low-pressure peritubular reabsorption—enables maximally efficient blood processing unmatched by single-capillary systems, refined across evolutionary time.
Location and Shape
The kidneys occupy the retroperitoneal space—posterior to peritoneal cavity—flanking the vertebral column bilaterally extending from approximately twelfth thoracic vertebra to third lumbar vertebra, with the right kidney positioned slightly more inferior than left due to superior displacement by hepatic mass occupying right upper quadrant. Each kidney exhibits the characteristic bean morphology instantly recognizable: smooth convex lateral border, concave medial border containing the hilum—the crucial entry and exit point for renal artery delivering blood, renal vein draining blood, ureter conducting urine, lymphatic vessels, and autonomic nerves—superior pole contacted by the adrenal gland, and inferior pole tapering caudally toward pelvis. Dimensions approximate 11-12 centimeters length, 5-7 centimeters width, 3 centimeters anterior-posterior thickness, weighing 120-170 grams in adults—roughly fist-sized yet containing architectural complexity rivaling organs ten times larger.
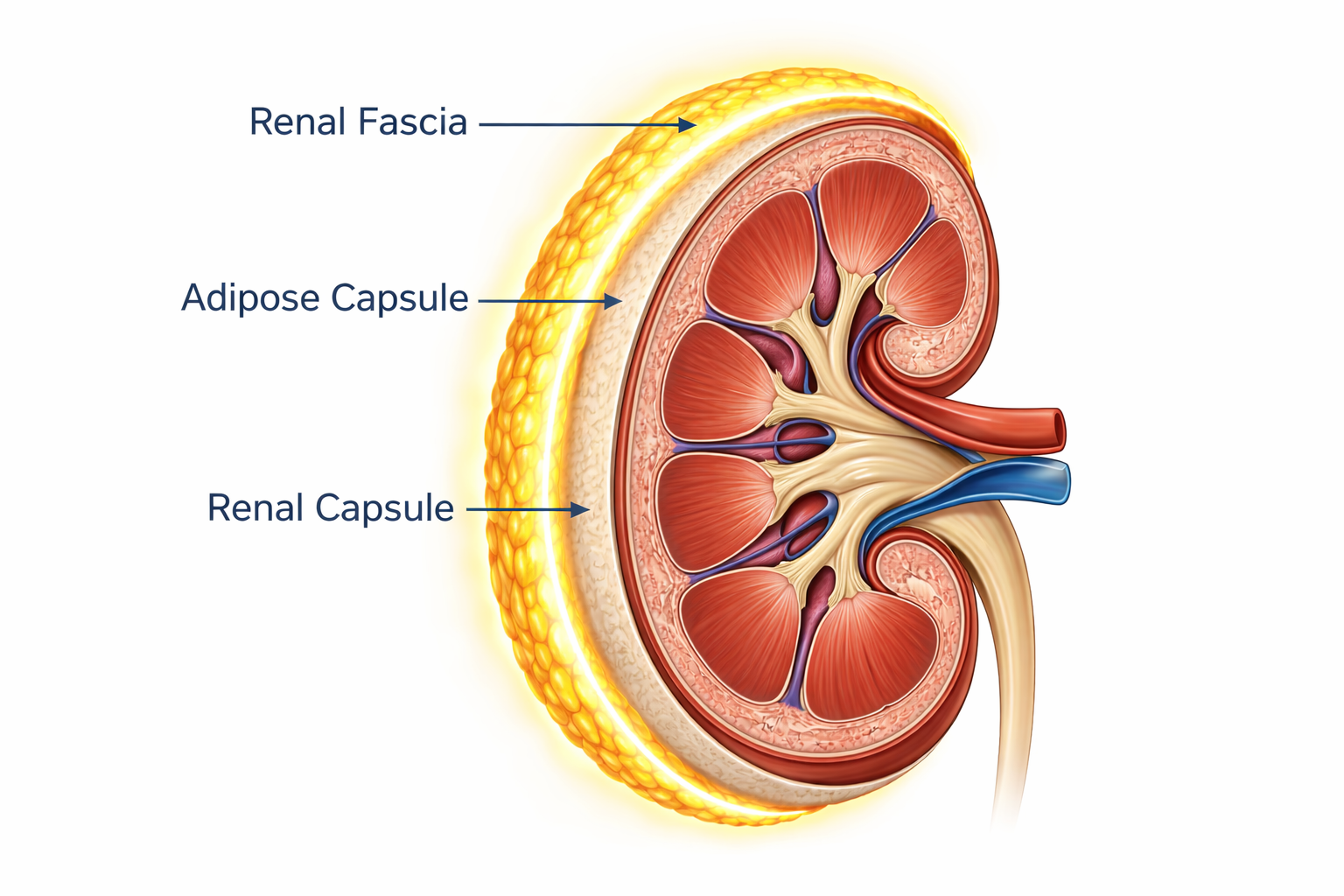
Three protective layers surround each kidney concentrically: innermost fibrous capsule providing tough adherent connective tissue envelope, middle perirenal fat layer cushioning and thermally insulating the organ, and outermost renal fascia (Gerota's fascia) anchoring kidneys firmly to posterior abdominal wall musculature while permitting slight movement during respiratory excursions. This posterior position beneath lower ribs, protected anteriorly by abdominal viscera and posteriorly by paraspinal muscles plus adipose tissue, shields these vital organs from anterior abdominal trauma while maintaining optimal vascular proximity to abdominal aorta and inferior vena cava for efficient blood access.
Diseases
Chronic kidney disease affects approximately 850 million individuals globally—exceeding the combined prevalence of diabetes and cancer—staged by estimated glomerular filtration rate measured in milliliters per minute per 1.73 square meters body surface area: Stage 1 equals ≥90 with kidney damage markers like proteinuria or hematuria, Stage 2 equals 60-89, Stage 3a equals 45-59, Stage 3b equals 30-44, Stage 4 equals 15-29, Stage 5 equals 15 requiring dialysis or transplantation for survival. Diabetic nephropathy constitutes the leading cause worldwide, resulting from chronic hyperglycemia inducing nonenzymatic glycation causing glomerular basement membrane thickening, mesangial matrix expansion, podocyte foot process effacement and injury, progressive glomerulosclerosis manifesting clinically as albuminuria exceeding 30 milligrams daily and progressively declining filtration rate. Hypertensive nephrosclerosis ranks second through relentless arteriolar sclerosis, ischemic glomerular damage, tubulointerstitial fibrosis creating vicious pathological cycles where kidney damage elevates blood pressure systemically, which accelerates further kidney injury perpetually.
 Acute kidney injury involves rapid filtration rate decline within hours or days from prerenal causes like hypoperfusion from volume depletion or heart failure, intrinsic renal causes like acute tubular necrosis from ischemia or nephrotoxins including aminoglycoside antibiotics, NSAIDs, radiocontrast media, or postrenal causes like urinary obstruction from stones or malignancy. Autosomal dominant polycystic kidney disease affects 1 in 400-1,000 individuals, progressively replacing normal parenchyma with fluid-filled cysts causing failure typically by age 50-60.
Acute kidney injury involves rapid filtration rate decline within hours or days from prerenal causes like hypoperfusion from volume depletion or heart failure, intrinsic renal causes like acute tubular necrosis from ischemia or nephrotoxins including aminoglycoside antibiotics, NSAIDs, radiocontrast media, or postrenal causes like urinary obstruction from stones or malignancy. Autosomal dominant polycystic kidney disease affects 1 in 400-1,000 individuals, progressively replacing normal parenchyma with fluid-filled cysts causing failure typically by age 50-60.
How to Protect the Kidneys
Kidney protection requires controlling modifiable risk factors aggressively and avoiding nephrotoxic exposures consistently throughout life. Glycemic control in diabetes maintaining hemoglobin A1c below 7% reduces diabetic nephropathy incidence and progression by 30-40% through multiple mechanisms; newer SGLT2 inhibitor medications provide additional renoprotection through reduced intraglomerular hyperfiltration pressure independent of glucose-lowering effects. Blood pressure control maintaining levels below 130/80 mmHg slows chronic kidney disease progression substantially, with renin-angiotensin system blockade using ACE inhibitors or angiotensin receptor blockers conferring renoprotective benefit beyond systemic pressure reduction through decreased proteinuria and reduced intraglomerular pressure. Adequate daily hydration producing urine output consistently exceeding 1.5 liters dilutes urinary solutes preventing kidney stone formation and facilitating metabolic waste elimination efficiently.
Dietary sodium restriction below 2,300 milligrams daily reduces blood pressure and proteinuria significantly. NSAIDs require strict minimization or complete avoidance due to prostaglandin synthesis inhibition reducing renal blood flow and risking acute kidney injury, particularly dangerous in elderly patients or those with preexisting volume depletion. Dietary protein intake moderation to approximately 0.8 grams per kilogram body weight daily in established kidney disease reduces hyperfiltration-induced glomerular injury. Regular aerobic exercise—minimum 150 minutes weekly moderate-intensity physical activity—improves glycemic control and blood pressure regulation protecting kidneys indirectly. Smoking cessation immediately halts tobacco-induced progressive endothelial dysfunction and oxidative stress accelerating disease. Early detection through screening high-risk populations using serum creatinine-based estimated glomerular filtration rate calculations and urine albumin-to-creatinine ratio measurements identifies disease when interventions maximally preserve remaining function.
Summary
The kidneys transcend simple waste filtration to emerge as supreme homeostatic regulators defending the infinitesimally narrow chemical composition separating living metabolism from thermodynamic equilibrium with the environment. Two million nephrons collectively process entire circulating blood volume forty times daily, filtering 180 liters of plasma while recovering 99% through molecular selectivity and transport efficiency unmatched by any human-engineered technology. They maintain blood pH within 0.05 units of 7.40—the difference between consciousness and coma—sustain electrolyte concentrations within milliequivalent ranges where deviation triggers cardiac arrest or neurological catastrophe, control blood volume and arterial pressure through integrated renin-angiotensin-aldosterone mechanisms, and synthesize essential hormones governing erythropoiesis, mineral metabolism, and cardiovascular tone affecting every organ system throughout the body.
Understanding these paired retroperitoneal organs—working ceaselessly, autonomously, flawlessly in darkness without conscious awareness—reveals the profound biological truth that complex organisms represent not singular entities but ongoing molecular negotiations between trillions of cells, and these fist-sized structures determine whether that negotiation continues or terminates. Each nephron executes thousands of independent transport decisions per second: which molecules salvage, which sacrifice, what concentration impose, what pH command—billions of integrated molecular calculations achieving the chemical stability permitting consciousness itself.
Protection requires consistent blood pressure control, optimal glycemic management, adequate hydration, sodium restriction, nephrotoxin avoidance, and early disease detection enabling timely interventions preserving irreplaceable nephron function. These silent guardians sustain the exact extracellular composition upon which every cellular process depends, separating treasure from waste, order from entropy, existence from oblivion.